ECR 2018 / C-2418
Decoding the Contrast Enhanced Brain
Congress:
ECR 2018
Poster Number:
C-2418
Type:
Educational Exhibit
Keywords:
Neoplasia, Infection, Education and training, Education, Contrast agent-intravenous, MR, Neuroradiology brain, Contrast agents
Authors:
V. B. Pai, K. Joshi, K. Gupta, C. Trivedi, A. Agrawal, B. Pai, R. Kharche, D. Lokhande; Mumbai/IN
DOI:
10.1594/ecr2018/C-2418

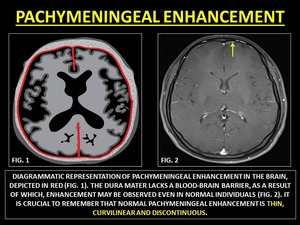
Fig. 6:
REPRESENTATIVE IMAGES OF PACHYMENINGEAL ENHANCEMENT

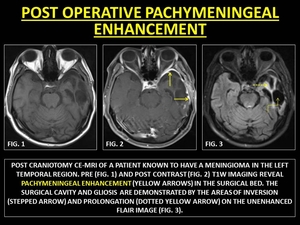
Fig. 7:
POST OPERATIVE PACHYMENINGEAL ENHANCEMENT

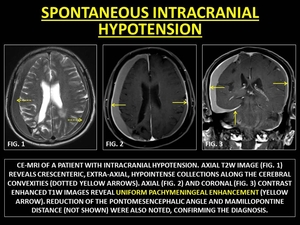
Fig. 8:
SPONTANEOUS INTRACRANIAL HYPOTENSION

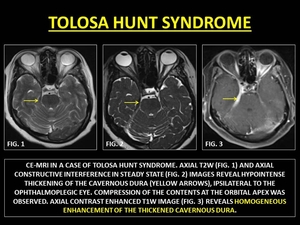
Fig. 9:
TOLOSA HUNT SYNDROME

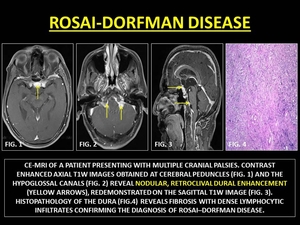
Fig. 10:
ROSAI-DORFMAN DISEASE

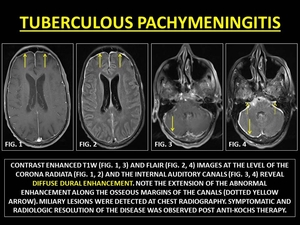
Fig. 11:
TUBERCULOUS PACHYMENINGITIS

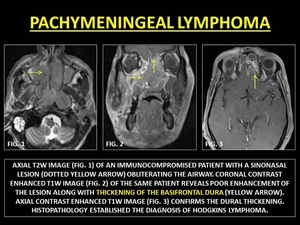
Fig. 12:
PACHYMENINGEAL LYMPHOMA

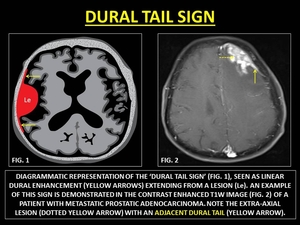
Fig. 13:
REPRESENTATIVE IMAGES OF 'DURAL TAIL SIGN'

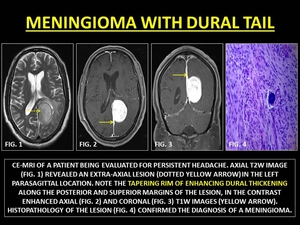
Fig. 14:
MENINGIOMA WITH DURAL TAIL

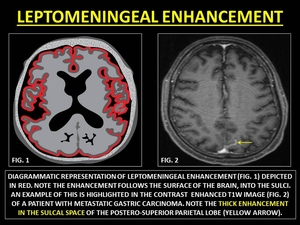
Fig. 15:
REPRESENTATIVE IMAGES OF LEPTOMENINGEAL ENHANCEMENT

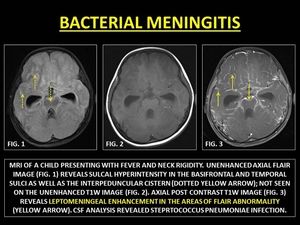
Fig. 16:
BACTERIAL MENINGITIS

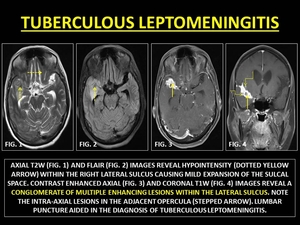
Fig. 17:
TUBERCULOUS LEPTOMENINGITIS

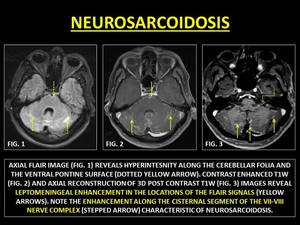
Fig. 18:
NEUROSARCOIDOSIS

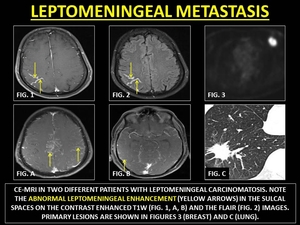
Fig. 19:
LEPTOMENINGEAL METASTASIS

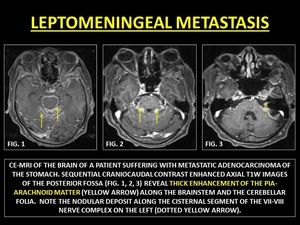
Fig. 20:
LEPTOMENINGEAL METASTASIS

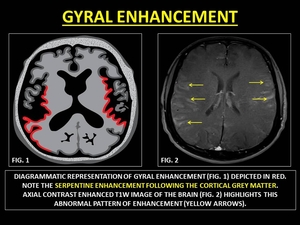
Fig. 21:
REPRESENTATIVE IMAGES OF GYRAL ENHANCEMENT

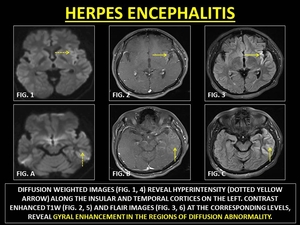
Fig. 22:
HERPES ENCEPHALITIS

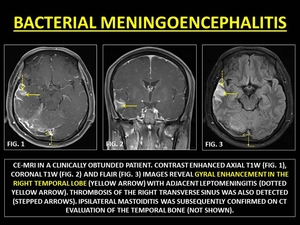
Fig. 23:
BACTERIAL MENINGOENCEPHALITIS

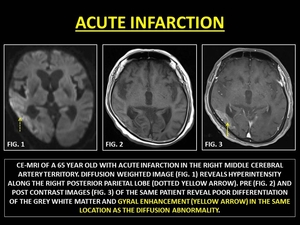
Fig. 24:
ACUTE INFARCTION

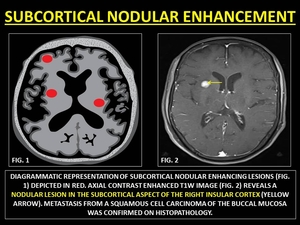
Fig. 25:
REPRESENTATIVE IMAGES OF SUBCORTICAL NODULAR ENHANCEMENT

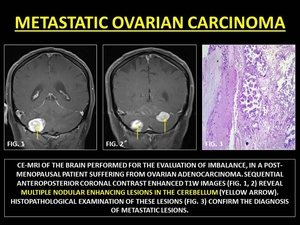
Fig. 26:
METASTATIC OVARIAN CARCINOMA

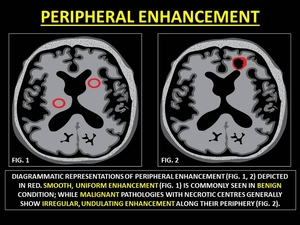
Fig. 27:
REPRESENTATIVE IMAGES OF PERIPHERAL ENHANCEMENT

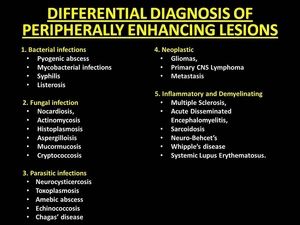
Fig. 28:
DIFFERENTIAL DIAGNOSIS OF PERIPHERALLY ENHANCING LESIONS

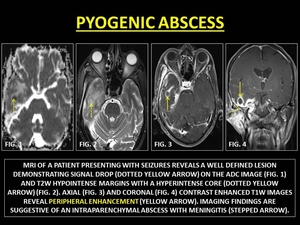
Fig. 29:
PYOGENIC ABSCESS

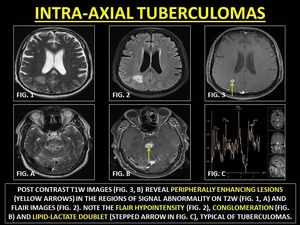
Fig. 30:
INTRA-AXIAL TUBERCULOMAS

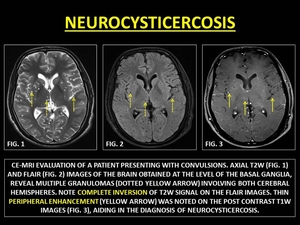
Fig. 31:
NEUROCYSTICERCOSIS

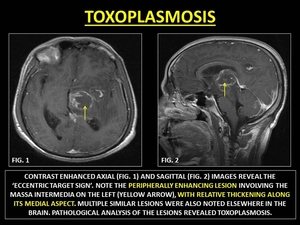
Fig. 32:
TOXOPLASMOSIS

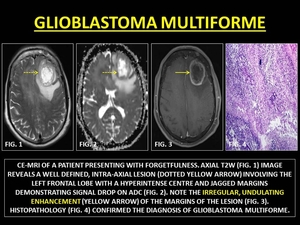
Fig. 33:
GLIOBLASTOMA MULTIFORME

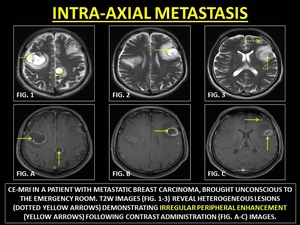
Fig. 34:
INTRA-AXIAL METASTASIS

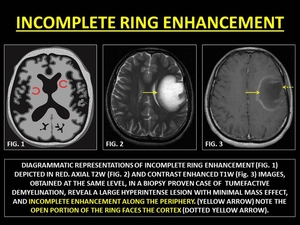
Fig. 35:
INCOMPLETE RING ENHANCEMENT

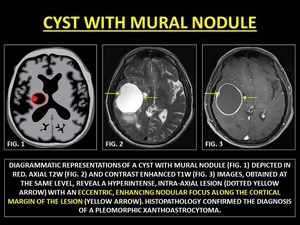
Fig. 36:
CYST WITH MURAL NODULE
 CONTRIBUTED BY DR. PRASHANT MUDGAL.")
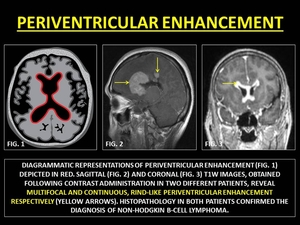
Fig. 37:
PERIVENTRICULAR ENHANCEMENT

Fig. 38:
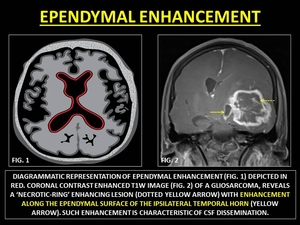
REPRESENTATIVE IMAGES OF EPENDYMAL ENHANCEMENT

Fig. 39:
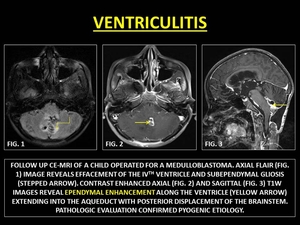
VENTRICULITIS

Fig. 40:
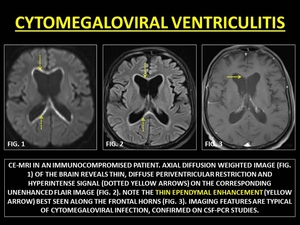
CYTOMEGALOVIRAL VENTRICULITIS

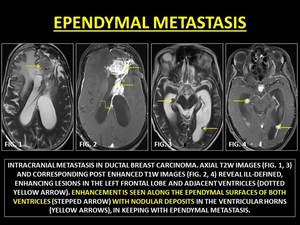
Fig. 41:
EPENDYMAL METASTASIS